Adenosine and Adenosine Receptors (The Receptors)
Free download. Book file PDF easily for everyone and every device. You can download and read online Adenosine and Adenosine Receptors (The Receptors) file PDF Book only if you are registered here. And also you can download or read online all Book PDF file that related with Adenosine and Adenosine Receptors (The Receptors) book. Happy reading Adenosine and Adenosine Receptors (The Receptors) Bookeveryone. Download file Free Book PDF Adenosine and Adenosine Receptors (The Receptors) at Complete PDF Library. This Book have some digital formats such us :paperbook, ebook, kindle, epub, fb2 and another formats. Here is The CompletePDF Book Library. It's free to register here to get Book file PDF Adenosine and Adenosine Receptors (The Receptors) Pocket Guide.
Contents:
The adenosine receptors or P1 receptors [1] are a class of purinergic G protein-coupled receptors with adenosine as endogenous ligand. The adenosine receptors are commonly known for their antagonists caffeine and theophylline , whose action on the receptors produces the stimulating effects of coffee , tea and chocolate.
Each type of adenosine receptor has different functions, although with some overlap. Most older compounds acting on adenosine receptors are nonselective, with the endogenous agonist adenosine being used in hospitals as treatment for severe tachycardia rapid heart beat , [9] and acting directly to slow the heart through action on all four adenosine receptors in heart tissue, [10] as well as producing a sedative effect through action on A 1 and A 2A receptors in the brain.
Adenosine Receptor Subtypes: Binding Studies
Xanthine derivatives such as caffeine and theophylline act as non-selective antagonists at A 1 and A 2A receptors in both heart and brain and so have the opposite effect to adenosine, producing a stimulant effect and rapid heart rate. Newer adenosine receptor agonists and antagonists are much more potent and subtype-selective, and have allowed extensive research into the effects of blocking or stimulating the individual adenosine receptor subtypes, which is now resulting in a new generation of more selective drugs with many potential medical uses.
Some of these compounds are still derived from adenosine or from the xanthine family, but researchers in this area have also discovered many selective adenosine receptor ligands that are entirely structurally distinct, giving a wide range of possible directions for future research.
- Yellowstone National Park Tour Guide.
- Differential equations.
- Frontiers | An emerging role for adenosine and its receptors in bone homeostasis | Endocrinology?
- Topoi (collected papers).
- Computer Methods for Mathematical Computations (Prentice-Hall series in automatic computation).
- GPCR Pathways - Issue No. 4!
- Ride the River The Sacketts Series, Book 5.
This receptor has an inhibitory function on most of the tissues in which it is expressed. In the brain, it slows metabolic activity by a combination of actions. Presynaptically, it reduces synaptic vesicle release while post synaptically it has been found to stabilize the magnesium on the NMDA receptor. Tecadenoson is an effective A 1 adenosine agonist, as is selodenoson. The A 1 , together with A 2A receptors of endogenous adenosine play a role in regulating myocardial oxygen consumption and coronary blood flow.
Stimulation of the A 1 receptor has a myocardial depressant effect by decreasing the conduction of electrical impulses and suppressing pacemaker cell function, resulting in a decrease in heart rate.
Bench-to-bedside review: Adenosine receptors – promising targets in acute lung injury?
This makes adenosine a useful medication for treating and diagnosing tachyarrhythmias , or excessively fast heart rates. This effect on the A 1 receptor also explains why there is a brief moment of cardiac standstill when adenosine is administered as a rapid IV push during cardiac resuscitation. The rapid infusion causes a momentary myocardial stunning effect.

In normal physiological states, this serves as a protective mechanism. However, in altered cardiac function, such as hypoperfusion caused by hypotension , heart attack or cardiac arrest caused by nonperfusing bradycardias , adenosine has a negative effect on physiological functioning by preventing necessary compensatory increases in heart rate and blood pressure that attempt to maintain cerebral perfusion. Adenosine antagonists are widely used in neonatal medicine ;.
A reduction in A 1 expression appears to prevent hypoxia-induced ventriculomegaly and loss of white matter, which raises the possibility that pharmacological blockade of A 1 may have clinical utility. Theophylline and caffeine are nonselective adenosine antagonists that are used to stimulate respiration in premature infants. Adenosine receptors play a key role in the homeostasis of bone. The A 1 receptor has been shown to stimulate osteoclast differentiation and function.
As with the A 1 , the A 2A receptors are believed to play a role in regulating myocardial oxygen consumption and coronary blood flow. The activity of A 2A adenosine receptor, a G-protein coupled receptor family member, is mediated by G proteins that activate adenylyl cyclase.
It is abundant in basal ganglia, vasculature and platelets and it is a major target of caffeine. The A 2A receptor is responsible for regulating myocardial blood flow by vasodilating the coronary arteries , which increases blood flow to the myocardium , but may lead to hypotension. Just as in A1 receptors, this normally serves as a protective mechanism, but may be destructive in altered cardiac function.
The role of A2A receptor opposes that of A1 in that it inhibits osteoclast differentiation and activates osteoblasts. This integral membrane protein stimulates adenylate cyclase activity in the presence of adenosine. This protein also interacts with netrin-1, which is involved in axon elongation.
- Major Legal Systems in the World Today.
- 3-Fabric Quilts. Quick Techniques for Simple Projects.
- Barrons Visual Dictionary: Italian: For Home, Business, and Travel.
- Stabat Mater, No. 10: Fac ut portem Christi mortem.
- Net-Centric Web Approaches to Intelligence and National Security.
Similarly to A2A receptor, the A2B receptor promotes osteoblast differentiation. It has been shown in studies to inhibit some specific signal pathways of adenosine.
Review ARTICLE
It allows for the inhibition of growth in human melanoma cells. The role of A3 receptor is less defined in this field. Studies have shown that it plays a role in the downregulation of osteoclasts. From Wikipedia, the free encyclopedia. Part of a series on Purinergic signalling Simplified illustration of extracellular purinergic signalling. Dhasmana, J.
Effect of adenosine deaminase inhibitors on the heart's functional and biochemical recovery from ischemia: a study utilizing the isolated rat heart adapted to 31 P nuclear magnetic resonance. Ely, S. Functional and metabolic evidence of enhanced myocardial tolerance to ischemia and reperfusion with adenosine. PubMed Abstract Google Scholar. Feoktistov, I.
Review ARTICLE
Role of adenosine A 2B receptors in inflammation. Adv Pharmacol. Frangogiannis, N. Regulation of the inflammatory response in cardiac repair. Givertz, M. The effects of KW, an adenosine A1-receptor antagonist, on diuresis and renal function in patients with acute decompensated heart failure and renal impairment or diuretic resistance. Goto, M. Adenosine infusion during early reperfusion failed to limit myocardial infarct size in a collateral deficient species. Google Scholar. Greenberg, B. Effects of multiple oral doses of an A1 adenosine antagonist, BG, in patients with heart failure: results of a placebo-controlled, dose-escalation study.
Regulation of inflammation by adenosine. Hasko, G. Adenosine receptors: therapeutic aspects for inflammatory and immune diseases. Nature Rev. Drug Disc. Headrick, J. Adenosine receptors and reperfusion injury of the heart. Ischaemic tolerance in aged mouse myocardium: the role of adenosine and effects of A1 adenosine receptor overexpression.
Homeister, J. Combined adenosine and lidocaine administration limits myocardial reperfusion injury. Circulation 82, — Humphrey, S. Improved functional recovery of ischemic myocardium by suppression of adenosine catabolism. Ingwersen, J. Dual roles of the adenosine A2a receptor in autoimmune neuroinflammation.
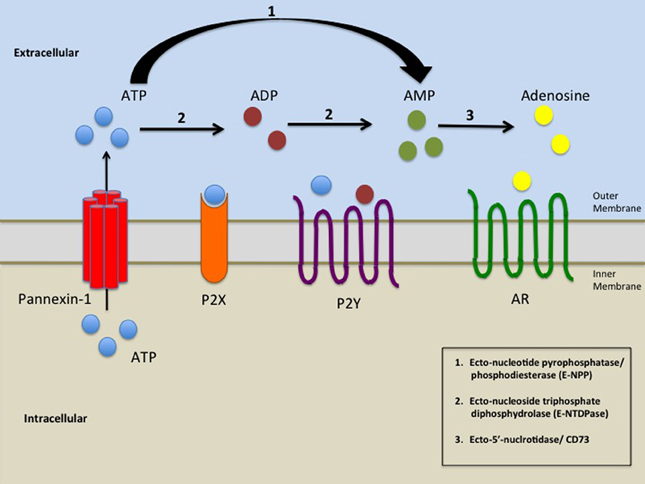
Adenosine receptors (ARs) comprise a group of G protein-coupled receptors ( GPCR) which mediate the physiological actions of adenosine. These effects are largely protective and are triggered by binding of adenosine to any of the four adenosine receptor subtypes namely A1, A2a, A2b, A3, which.
Jacobson, K. Medicinal chemistry of adenosine, P2Y and P2X receptors. Neuropharmacology , 31— Karmouty-Quintana, H. Adenosine A2B receptor and hyaluronan modulate pulmonary hypertension associated with chronic obstructive pulmonary disease. Cell Mol. Adenosine signaling during acute and chronic disease states. The A2B adenosine receptor modulates pulmonary hypertension associated with interstitial lung disease. Kloner, R. Heart J.
Kolachala, V. Blockade of adenosine A2B receptors ameliorates murine colitis. Koupenova, M.
Ligands for Adenosine Receptors - Jena Bioscience
A2b adenosine receptor regulates hyperlipidemia and atherosclerosis. Kristo, G. Aged rat myocardium exhibits normal adenosine receptor-mediated bradycardia and coronary vasodilation but increased adenosine agonist-mediated cardioprotection. A Biol. Krumholz, H. Reduction in acute myocardial infarction mortality in the United States: risk-standardized mortality rates from JAMA , — Lasley, R.
Beneficial effects of the adenosine A 2a agonist CGS in infarcted and stunned porcine myocardium.
- Deadly Angel: The Bizarre True Story of Alaskas Killer Stripper
- Secret Language of Business - How to Read Anyone in 3 Seconds or Less
- W.H.A.M.
- Exploring Developmental Psychology
- Delta Blues: The Life and Times of the Mississippi Masters Who Revolutionized American Music
- Your Tax Dollars at Work: The Implications of Taxpayer-funded Lobbying
- Obstruction Theory: on Homotopy Classification of Maps