Towards the Neurobiology of Chronic Pain (Progress in Brain Research)
Free download. Book file PDF easily for everyone and every device. You can download and read online Towards the Neurobiology of Chronic Pain (Progress in Brain Research) file PDF Book only if you are registered here. And also you can download or read online all Book PDF file that related with Towards the Neurobiology of Chronic Pain (Progress in Brain Research) book. Happy reading Towards the Neurobiology of Chronic Pain (Progress in Brain Research) Bookeveryone. Download file Free Book PDF Towards the Neurobiology of Chronic Pain (Progress in Brain Research) at Complete PDF Library. This Book have some digital formats such us :paperbook, ebook, kindle, epub, fb2 and another formats. Here is The CompletePDF Book Library. It's free to register here to get Book file PDF Towards the Neurobiology of Chronic Pain (Progress in Brain Research) Pocket Guide.
Contents:
This can teach us a lot about the nature of the experiences that patients are going through and help us understand how the chronic pain experience is generated. It also helps us identify areas of the brain that we could target with treatments like psychotherapy or drug therapy, and understand the vulnerabilities that these patients run into, such as overeating or getting hooked on opioid pills.
How did you initially become interested in science, and then more specifically in chronic pain research?
Before medical school, I went into philosophy for a year, and I was really interested in the Philosophy of Mind. In medical school, I was very drawn to understanding how the brain comes up with the mind. My interest in chronic pain happened by accident.
A Future Without Chronic Pain: Neuroscience and Clinical Research
I had a professor in medical school that was working on pain and neuroimaging in Chicago, and so I ended up in Dr. At the time, brain imaging was still in its early years, and we were doing all these cross-sectional studies just to understand what's going on in the brain of patients with chronic pain. And, interestingly enough, almost 15 years ago, we started noticing that the areas of the brain that respond the most to analgesic drugs were also involved in emotion processing, or what we call the limbic system.
Are there any departments or centers at UR that you're looking forward to collaborating with? Neurosurgery, Orthopedics, Neurology, the Eastman Institute for Oral Health EIOH … Pain is a complaint that is common to many, many different diseases, and chronic pain can occur in multiple systems in the body. Despite almost 25 years of brain imaging, we still don't understand a lot of chronic pain conditions.
Since I focus a lot on chronic back pain, I will be working closely with Dr. John Markman in Neurology and Neurosurgery, and Dr. Robert Dworkin in Anesthesiology. The different departments offer crucial and critical collaboration that will help me translate some of my ideas into the clinic. Another collaboration I'm really looking forward to is working with people who have chronic temporomandibular joint TMJ pain, which is a chronic pain of the joint between the cranium and the mandible lower jaw.
Thus the patient continues to experience pain, even with less provocation [8]. However other research has suggested that sensitization may develop from: activity-dependent synaptic plasticity, gap junctions, astrocytes, membrane excitability and gene transcription. However it has been proposed that there may be one of two reasons for its development, although there is no conclusive evidence to support this: [8] Pre-existing factors genetics that may predispose an individual to have altered central nervous system functioning following injury Factors environmental that may cause altered central nervous system functioning once injury has occurred.
The biomedical model is most commonly used by physiotherapists and other medical health professionals for the management of pain. Nerves were connected to the brain as a piece of rope may be connected to an alarm; thus as pulling of the rope would cause.
Descartes model continues to be used in current medical practice and influences the perception that all pain is a result of injury and tissue damage. However Descartes biomedical model has been questioned in recent years, with critics arguing that it fails to consider the perception of pain from the nervous system, as well as the psychological and social factors that may influence recovery.
The examples below suggest that pain may potentially be a phenomenon more than just nociception, and may have a neurological element:. This example therefore proposes that the patient's beliefs emotions and past experiences of pain can alter the brains interpretation of the pain. However the validity of study findings must be questioned, as investigations were conducted 60 years ago, thus may be significantly outdated. Furthermore the study did not consider the effect of shock or adrenaline, which has been proposed to influence immediate pain responses.
In the last century Descartes biomedical model has been replaced by the biopsychosocial model of chronic pain [13] , in which pain is classified as being due to increased sensitivity of the nervous system rather than further injury. PNE first of all puts the complex process of describing the nerves and brain into a format that is easy to understand for everyone; no matter whether the target audience is of a particular age, educational level or ethnic group. Methods of PNE delivery vary but can typically involve around 4 hours of teaching that is provided to a group or individually, either in single or multiple sessions.
IN ADDITION TO READING ONLINE, THIS TITLE IS AVAILABLE IN THESE FORMATS:
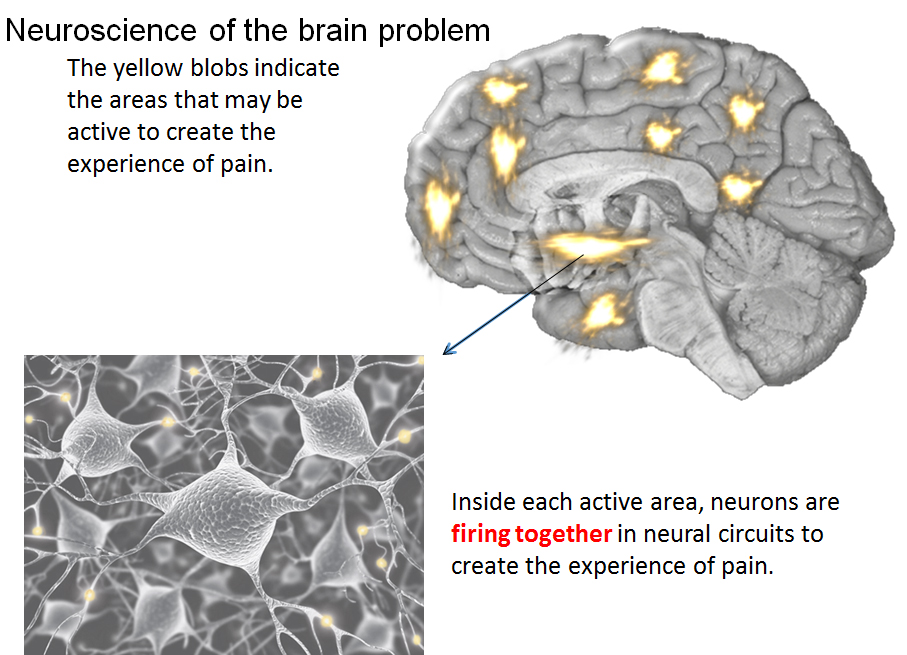
Figure 6. It is such an example that helps patient to break away from a view of a particular tissue being the issue e. Figure 7. There are various types of brain imaging to show brain activity in pain states, some scans of which are pictured below:. The effects of decreased pain related brain activity are measurable via brain imaging as demonstrated in the example below:. Areas of brain activity related to pain were demarcated in red.
Note no red areas. These images demonstrated brain activity related to pain whereby larger areas of red signifies more pain related activity, hence more pain. Figure row 3 - after initial scans the patient was taken out of the scanner and provided with a teaching session about pain for minutes.
Following this, the scan of the patient was immediately repeated doing the same painful task as performed in Row 2.
- The Official ScratchJr Book: Help Your Kids Learn to Code.
- Pain neuroscience education on YouTube [PeerJ].
- Q&A with Paul Geha, M.D..
- Pain & the Neuroscience of Suffering | Center for Law, Brain and Behavior.
- Strategies to Ameliorate Oxidative Stress During Assisted Reproduction.
Note this time however, there was significantly less activity fewer red areas despite performing the same movement. There is an obvious link with patient catastrophising thoughts and pain related brain activity, shown by the immediate reduction in brain activity following PNE provision in the above example. Furthermore, there is a link in attention to pain that when negatively perceived, impacts on the experience of pain being greater.
A comparison of the effects of 2 types of massage and usual care on chronic low back pain: A randomized, controlled trial. Annals of Family Medicine 9 3 Therefore, if functional movement exacerbates the pain symptoms, a chronic pain patient should not try to push through the pain in that moment. Brain networks predicting placebo analgesia in a clinical trial for chronic back pain. Chen, X.
However, in this population there is less reporting of pain and analgesic use. Is this due to difficulty to communicate pain or due to reduced attention to pain?
Cognitive Neurology
A recent systematic review investigating the benefits of pain neuroscience education PNE , discovered that PNE significantly decreased pain, pain catastrophisation and perceived disability compared to the control group ongoing medical care , in both the short and long-term. Although the review searched all major databases, only 8 studies were included in the review, with all included studies having either good, very good or excellent methodological quality.
- You are here.
- Towards the Neurobiology of Chronic Pain, Volume 110.
- Improving Learning in a Professional Context: A Research Perspective on the New Teacher in School.
- Brain imaging is illuminating the neural patterns behind pain’s infinite variety..
- Research and Discovery at the Neurosciences Center.
The internal validity of the study is positive with measures in place to reduce risk of bias where possible. Methodological quality could have only improved through blinding but is not appropriate for the groups. Sample size powered.
- Global Governance, Economy and Law: Waiting for Justice (Routledge Studies in International Law, 4).
- What the Science of Touch Says About Us.
- Iowa Neuroscience Institute.
- The Way of All Flesh (Giant Thrifts).
The secondary outcomes improving patient experiences after surgery and health utilisation are hugely clinically relevant, especially in relation to the financial challenges of National Health Service NHS in the UK. Any reduction in services post-surgery and thus reducing costs, whilst additionally improving patient experiences with minimal cost to implement cannot be overlooked.