Progressive Multiple Sclerosis
Free download. Book file PDF easily for everyone and every device. You can download and read online Progressive Multiple Sclerosis file PDF Book only if you are registered here. And also you can download or read online all Book PDF file that related with Progressive Multiple Sclerosis book. Happy reading Progressive Multiple Sclerosis Bookeveryone. Download file Free Book PDF Progressive Multiple Sclerosis at Complete PDF Library. This Book have some digital formats such us :paperbook, ebook, kindle, epub, fb2 and another formats. Here is The CompletePDF Book Library. It's free to register here to get Book file PDF Progressive Multiple Sclerosis Pocket Guide.
Contents:
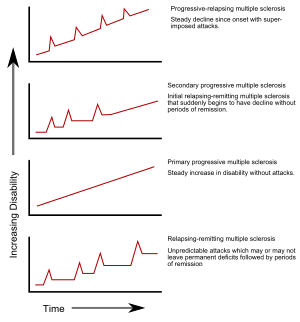
The progressive worsening of symptoms is caused by nerve damage or loss rather than the inflammation. The symptoms of primary-progressive multiple sclerosis are similar to those of secondary-progressive multiple sclerosis.
Microglia activation a. Progressive multiple sclerosis and gray matter pathology: an MRI perspective. The sponsor has recently voluntarily terminated the study. Despite our increasing knowledge and better understanding of the underlying mechanisms, many questions remain open. Mult Scler 20 11 — You can login by using one of your existing accounts.
The main symptom of both forms of the condition is a gradual worsening of disability. Ten percent of all multiple sclerosis patients are diagnosed with PPMS. The cause of PPMS is unknown. Patients with PPMS tend to be diagnosed in their mid-to-late 30s. The condition affects men and women equally.
Diagnosis of all forms of MS begins with a detailed medical history and neurological examination. Because MS can have similar symptoms of other nervous system disorders, diagnostic tests help rule out other causes and confirm a diagnosis. These tests may include a magnetic resonance imaging MRI scan of the brain and spinal cord. The patient's medical team may order a lumbar puncture, also known as a spinal tap, and cerebrospinal fluid analysis, as well as nerve function tests. Blood tests may be performed to rule out other conditions that have similar symptoms.
The only definitive way to diagnose PPMS apart from other forms of multiple sclerosis is by observation. Although the FDA has approved medications for relapsing-remitting forms of the disease, there are currently no approved medications for PPMS. Treatment of PPMS is focused on managing the symptoms and increasing daily functioning. Symptoms of PPMS can affect a patient's daily life, so physical and occupational therapy may be used to manage symptoms and help patients adjust to living and working situations.
Choosing the right medication requires careful consideration of the risks and benefits, along with close collaboration with an experienced neurologist with experience in treating the disease, such as those at the Multiple Sclerosis Center in Cedars-Sinai's Department of Neurology. All Rights Reserved. A c 3 non-profit organization.
The translations may include errors or change the intended meaning of the text.
Ann Neurol 68 , — Komori, M. Cerebrospinal fluid markers reveal intrathecal inflammation in progressive multiple sclerosis. Pathogenic mechanisms associated with different clinical courses of multiple sclerosis. Schenkel, J. Tissue-resident memory T cells. Immunity 41 , — Kapoor, R. Effect of natalizumab on disease progression in secondary progressive multiple sclerosis ASCEND : a phase 3, randomised, double-blind, placebo-controlled trial with an open-label extension.
related stories
Lancet Neurol. Greenwood, J.
Statin therapy and autoimmune disease: from protein prenylation to immunomodulation. Inflammopharmacology 23 , — Zhang, X. Paintlia, A. HMG-CoA reductase inhibitor augments survival and differentiation of oligodendrocyte progenitors in animal model of multiple sclerosis. Wang, J. Statins for multiple sclerosis. Cochrane Database Syst.
Chataway, J. Effect of high-dose simvastatin on brain atrophy and disability in secondary progressive multiple sclerosis MS-STAT : a randomised, placebo-controlled, phase 2 trial. Chan, D.
Effect of high-dose simvastatin on cognitive, neuropsychiatric, and health-related quality-of-life measures in secondary progressive multiple sclerosis: secondary analyses from the MS-STAT randomised, placebo-controlled trial. Kurte, M. Rice, C. Safety and feasibility of autologous bone marrow cellular therapy in relapsing-progressive multiple sclerosis. Connick, P. Autologous mesenchymal stem cells for the treatment of secondary progressive multiple sclerosis: an open-label phase 2a proof-of-concept study.
Assessment of bone marrow-derived cellular therapy in progressive multiple sclerosis ACTiMuS : study protocol for a randomised controlled trial. Trials 16 , Mancardi, G. Autologous hematopoietic stem cell transplantation in multiple sclerosis: a phase II trial. Neurology 84 , — Burt, R. Effect of nonmyeloablative hematopoietic stem cell transplantation vs continued disease-modifying therapy on disease progression in patients with relapsing-remitting multiple sclerosis: a randomized clinical trial.

Muraro, P. Long-term outcomes after autologous hematopoietic stem cell transplantation for multiple sclerosis. JAMA Neurol. A meta-analysis of studies investigating stem cell transplantation in MS. Michel, L. B cells in the multiple sclerosis central nervous system: trafficking and contribution to CNS-compartmentalized inflammation. Pollinger, B. Li, R. Transl Med. Magliozzi, R. B-cell enrichment and Epstein-Barr virus infection in inflammatory cortical lesions in secondary progressive multiple sclerosis. Howell, O. Meningeal inflammation is widespread and linked to cortical pathology in multiple sclerosis.
A key neuropathological study, demonstrating the link between meningeal inflammation and cortical neurodegeneration.
Choi, S. Meningeal inflammation plays a role in the pathology of primary progressive multiple sclerosis. A gradient of neuronal loss and meningeal inflammation in multiple sclerosis. Romme Christensen, J. Systemic inflammation in progressive multiple sclerosis involves follicular T-helper, Th and activated B-cells and correlates with progression.
The clinical subtypes of multiple sclerosis: a new classification.
Blauth, K. Antibodies produced by clonally expanded plasma cells in multiple sclerosis cerebrospinal fluid cause demyelination of spinal cord explants.
Rojas, O. Recirculating intestinal IgA-producing cells regulate neuroinflammation via IL Cell , — Atacicept in multiple sclerosis ATAMS : a randomised, placebo-controlled, double-blind, phase 2 trial.
- Collected Problems in Numerical Methods
- Language Acquisition across Linguistic and Cognitive Systems (Language Acquisition and Language Disorders)
- The Interrogation of Joan of Arc
- A Companion to Greek Literature (Blackwell Companions to the Ancient World)
- Fostering Public-private Partnership for Innovation in Russia
- The Price of Freedom: A History of East Central Europe from the Middle Ages to the Present
- Introduction to Quality and Safety Education for Nurses: Core Competencies